
Thirteen years. That is how long I have been here.
You have carried me through every appointment. The orthopedic surgeon who said the MRI was clean. The rheumatologist who could not explain why the labs kept returning normal. The pain specialist who offered a diagnosis that meant, effectively, "we don't know." You have described me to more physicians than you can count. You have filled questionnaires about my intensity, my character, my timing. You have given me a number, on scales from one to ten, every morning for thirteen years.
And every time, the structural tests came back normal.
That is not because I was not there. I was always there. The problem is that no one was looking in the right place.
The Gap Between Structure and Function
Modern diagnostic imaging is extraordinarily good at one thing: finding structural abnormalities. An MRI will identify a herniated disc, a torn ligament, an inflamed joint. It maps anatomy with remarkable precision.
What it cannot map is physiology. It cannot show whether nerves are firing correctly, whether the autonomic nervous system is regulating vascular tone as it should, or whether microvascular circulation in a painful region is responding to stimuli the way a healthy nervous system would.
This is not a failure of imaging technology. It is a fundamental mismatch between the question being asked and the tool being used to answer it. When a patient's pain is driven by autonomic dysregulation rather than structural damage, structural imaging will, by design, find nothing.
For a significant portion of patients presenting with chronic pain, that mismatch is the entire story.
Research has consistently found that up to 85% of chronic low back pain cases cannot be attributed to a specific structural diagnosis. Studies of small-fiber neuropathy have demonstrated that patients with severe neuropathic symptoms frequently return normal nerve conduction study results, because standard electrophysiology primarily evaluates large-fiber function. Autonomic nervous system disorders can produce debilitating pain in patients whose conventional workups return entirely clean.
These patients are not imagining their symptoms. They are producing a physiological signal that standard tests are not equipped to receive.
What the Cold Stress Test Heard
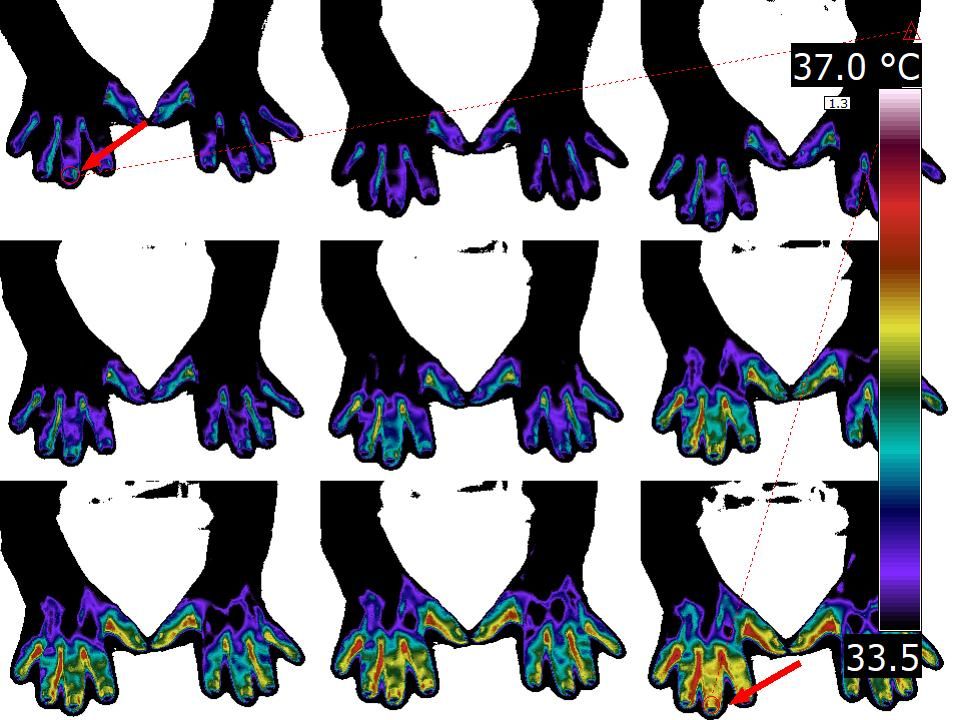
The cold stress provocative test is a thermal imaging protocol that evaluates the functional integrity of the autonomic nervous system by observing vascular response to a controlled cold stimulus.
Here is what a healthy response looks like: when exposed to cold, peripheral vasculature constricts, skin temperature drops, and on subsequent rewarming, temperature returns symmetrically and within a predictable time window. The autonomic nervous system orchestrates this entire sequence. It is measurable, observable, physiological behavior.
Autonomic dysfunction disrupts that behavior in detectable ways.
A paradoxical hyper-radiation response presents as abnormal thermal elevation rather than the expected cooling in the affected region, following the cold stimulus. Instead of vasoconstriction, the tissue shows evidence of dysregulated vascular tone — a circulatory response that the autonomic nervous system is failing to modulate correctly. This deviation is visible in the thermal image as a pattern inconsistent with normal autonomic regulation.
This is not a subjective finding. It is not a pain rating on a numeric scale. It is a thermal pattern, captured by an infrared sensor, reflecting what the nervous system is actually doing in real time.
In a recent case documented by Dr. Carlos Dalmaso, a clinical thermography specialist, a patient with thirteen years of normal structural imaging underwent cold stress thermal assessment. The result was a paradoxical hyper-radiation response in the affected region: objective thermal evidence of autonomic dysfunction that had been generating physiological signals throughout every prior scan that returned normal.
The pain was never imaginary. It was autonomic. And it was measurable.
Why Structural Imaging Has This Blind Spot
Every diagnostic tool has a defined scope. MRI produces high-resolution images of anatomical structures. X-ray shows bone density and alignment. CT maps tissue density. These are powerful tools for the questions they are designed to answer.
Autonomic function is not a structural question. It is a regulatory question: how is the nervous system managing vascular tone, temperature regulation, and peripheral circulation? Is the response to a physiological challenge normal or dysregulated?
No structural scan answers that question. Not because the scans are inadequate at what they do, but because they are doing something fundamentally different.
Infrared thermal imaging captures surface temperature patterns that reflect underlying circulatory and metabolic activity. When combined with a controlled functional challenge like the cold stress test, it creates a window into the dynamic behavior of the autonomic nervous system that anatomical imaging cannot provide. The thermal camera is not competing with the MRI. It is asking a question the MRI was never built to ask.
For patients whose pain originates from functional dysregulation rather than structural damage, that is the difference between thirteen more years of "normal results" and a first piece of objective clinical evidence.
Where This Matters Most
The patient population most likely to benefit from cold stress thermal assessment includes individuals presenting with:
- Chronic pain that does not map to structural findings on imaging
- Symptoms consistent with small-fiber neuropathy, with normal nerve conduction studies
- Complex regional pain syndrome (CRPS) at any stage of clinical evaluation
- Autonomic dysfunction syndromes with peripheral manifestations
- Unexplained pain following soft tissue injury where structural recovery appears complete
In these populations, the cold stress thermal response supports a more accurate characterization of pain mechanism, informs treatment direction, and provides the patient with objective evidence that validates their experience.
For a patient who has been told for thirteen years that all their tests are normal, that validation carries clinical weight that should not be underestimated. Establishing an objective basis for pain that has been dismissed by structural imaging changes the trajectory of care. It shifts the clinical conversation from "we cannot find anything wrong" to "here is what we found, and here is what it means."
That shift matters. Not just diagnostically. To the patient who has spent a decade being told their body is fine when their body has been anything but.
The Signal That Was Always There
I was never silent.
Every morning I produced a signal. Every moment of dysregulated vascular tone was a data point. Every paradoxical response to cold was a measurable deviation from normal autonomic behavior. The instruments used to look for me were not designed to detect that kind of signal. They were looking for structure. I am not a structural problem.
Thermal imaging did not discover me. It listened in the right frequency.
For clinicians working with patients who carry years of "normal" results, this is the core implication: the absence of structural findings is not the same as the absence of pathology. When the nervous system is the source of the signal, the assessment must be capable of reading the nervous system's language.
The cold stress thermal test is one way to do that. It is objective, non-invasive, and capable of revealing autonomic dysregulation that no MRI, no X-ray, and no nerve conduction study will surface.
When structure says nothing, function may still have everything to say.
Vizbodx Inc. is developing AI-powered infrared medical imaging technology designed to detect asymmetric thermal patterns in pain management, neuropathic assessment, and occupational health — often before symptoms have a conventional diagnosis to attach to.
Recovery begins with discovery.
→ Read the original clinical case by Dr. Carlos Dalmaso on LinkedIn → Learn more about Vizbodx
References
- Dalmaso C. Clinical case: 13-year chronic pain patient, cold stress provocative thermal testing. LinkedIn, March 2026. https://www.linkedin.com/in/dalmasont/
- Wolfe F, et al. The Fibromyalgia Syndrome: a consensus report on fibromyalgia and disability. J Rheumatol. 1996.
- Oaklander AL, et al. Objective evidence that small-fiber polyneuropathy underlies some illnesses currently labeled as fibromyalgia. Pain. 2013 Nov;154(11):2310-6. https://pubmed.ncbi.nlm.nih.gov/23748115/
- Bruehl S. Complex regional pain syndrome. BMJ. 2015 Jul 29;351:h2730. https://www.bmj.com/content/351/bmj.h2730
- Low PA, et al. Laboratory findings in reflex sympathetic dystrophy: a preliminary report. Clin J Pain. 1994;10(3):235-9.